Painting: Renoir, Pierre-Auguste. (1880-1). Luncheon of the Boating Party, Washington DC: The Phillips Collection.
“I cannot remember the books I’ve read any more than the meals I have eaten; even so, they have made me.” ― Ralph Waldo Emerson
I initially set myself the goal of reading one book per week for 2016, and although a pair of books I’ll mention below kept me from reaching my goal, I was able to read (and thanks to Audible, listen to) a ton of great books this year. (Follow what I’m reading on Goodreads). Below are the best five books (and one documentary) that I came across this year.
Fiction
I’m not typically a big fan of fiction, so I only have one suggestion here. I heard Chris Sacca recommend How to Get Filthy Rich in Rising Asia by Mohsin Hamid on two separate occasions, so I had to check it out. For this one, I listened to the Audible version, since it was narrated by the author. This is a novel written in the style of a self-help book, giving a dark, first-person account of a nameless poor boy who becomes a wealthy tycoon.
Non-fiction: History and the Future
Sapiens: A Brief History of Humankind by Yuval Noah Harari followed by Superintelligence: Paths, Dangers, Strategies by Nick Bostrom. These are the two long, dense books that kept me from my goal of a book per week, but it was completely worth it. Sapiens (464 pages) gives an overview of human history through the perspective of four different revolutions: cognitive, agricultural, and scientific, and will improve your understanding of how Homo sapiens have been able to survive, thrive and conquer. Superintelligence (390 pages) takes a look at the current state of artificial intelligence, how a superintelligenece will eventually form (it’s inevitable), and ideas on how we should develop these systems to maintain control.
Non-fiction: Personal Development
Extreme Ownership: How U.S. Navy SEALs Lead and Win by Jocko Willink and Leif Babin and Ego Is the Enemy by Ryan Holiday. In the author’s own words, Extreme Ownership: “explains the SEAL leadership concepts crucial to accomplishing the most difficult missions in combat and how to apply them to any group, team, or organization.” I suggest pairing this book with Ego Is the Enemy, which uses underpinnings in stoic philosophy and well selected stories to teach the reader to: “Forget yourself and focus on the work. Be humble and persistent. Value discipline and results, not passion and confidence. Be lesser, do more” (from Derek Sivers editorial review).
Documentaries
Somm (available on Netflix and iTunes) follows four people trying to pass the Master Sommelier Diploma, a title currently only earned by 233 people in the world. Beyond the wine knowledge displayed in this movie, this documentary is also a look at what it takes to become the best of the best in a field, and resembles Jiro Dreams of Sushi in the depth of mastery displayed.
Image by AaronMosh7 (Own work) [CC BY-SA 3.0], via Wikimedia Commons.
“Consider getting smaller in order to get bigger.” — Sir Richard Branson
Many people feel a bit of overwhelm at the idea of using social media during a medical meeting. These same people are recognizing the many benefits of using social media: connecting with others, actively learning, and promoting their work.
(This post is going to focus on using Twitter efficiently, but if you’re interested in digging deeper into what you can do, take a look at my talk from the 2016 ACR Program Directors’ Conference: Using Twitter in Medical Education and links to prior social media summaries from ACR 2014 and ACR 2015.)
Using Twitter during the meeting doesn’t have to be difficult or significantly time consuming.
After you’re following everyone at the meeting, use the Nuzzel website or app (iOS | Android) to catch up on highlights from people you’re following from the last 24 or 48 hours, (which shows the most important tweets in your timeline, according to RTs and likes). It can also send you a daily email that you can review later. (For more details, see my prior post about how I keep myself on a low information diet using Nuzzel).
If you’re using a laptop at the meeting, try using tchat.io on your web browser to more efficiently follow and participate in the #ACR16 hashtag in real-time. Bonus: tchat.io will automatically include the hashtag in your tweets so that you’re included in the conversation.
“Tell me and I forget, teach me and I may remember, involve me and I learn.” — Benjamin Franklin
The ACR Annual Meeting (#ACR16) is such a huge event that it’s worth your time to spend an hour or two planning your time at the meeting. (I highly suggest Dr. Philip Gardiner’s post: How to make the most of a medical conference….)
At this point, I generally attend sessions that I want to talk to the speaker afterwards, and make note of other sessions that I want to watch later online through SessionSelect.
Besides this, I suggest scheduling some time every day to exercise during the meeting. Really: put it in your calendar. (Alternatively: schedule a caffeine nap.)
Here’s my tentative #ACR16 session schedule:
Saturday, November 12:
8am–4pm: ACR Review Course. Always a well selected group of topics relevant to clinicians.
7:30–8:30am: Year in Review. Summary of the best in clinicial and basic science research of the last year. Happy to see Dr. Ingrid Lundberg from the Karolinska Institutet will be giving the clinical portion this year.
9:00–11:00am: I’ll be helping present #RheumJC’s poster #1145: #Rheumjc: Impact of Invited Authors on a Twitter Based Rheumatology Journal Club. Check RheumJC.com on the day of the poster for a downloadable pdf of our poster. Better yet: come say hi to the #RheumJC team.
2:30–4:00pm: Innovative Solutions to Deliver Care. Two interesting back to back lectures. The first, by Dr. Rafael Grossmann (@ZGJR), part of Singularity University’s Exponential Medicine and the first surgeon to use Google Glass during a live surgery. The second, by my friend, Dr. Irwin Lim (@_connectedcare), discussing his experiences with telerheumatology.
Official session overview:The tweet up is an informal event without an agenda organized by ACR members. It is an opportunity for members who engage on Twitter to meet face-to-face. All annual meeting attendees are welcome to participate. The tweet up is designed to facilitate personal connections within the international rheumatology community.
Twitter continues to be the gold standard social media tool for physician lifelong learning, which I’ve spoken about earlier this year at the 2016 ACR Program Directors’ Conference: Using Twitter in Medical Education.
The use of social media in medicine has continued to mature. Major medical meetings now have social media as a centerpiece for discussion, indexed on Symplur’s Healthcare Hashtag Project. Online journal clubs have organized, such as our very own #RheumJC, holding monthly sessions with participation of authors to directly answer questions about their articles.
There is a growing interest in documenting the use of Twitter at medical meetings. “Tweeting the meeting” has many benefits, including enhancing the educational experience of meeting attendees, disseminating content to those not in attendance (physicians, patients, general public and the media), and increasing the visibility of the medical organization. While still seen by many as frivolous, an increasing number of physicians and organizations understand the real value that comes from an active social media presence during conferences.
”What gets measured, gets managed.” – Peter Drucker
Despite being considered one of the techie people in the physician/rheumatology community and a self-proclaimed Apple fanboy, it might be surprising to know that I don’t own (or want) an Apple Watch.
But the main reason I don’t own any type of smartwatch is that I don’t see anything useful that they allow me to track.
When I look for things to track, I look for key performance indicators (KPIs): things that I consider modifiable activities, that when tracked or measured, correlate with improvement in specific goals.
With this in mind, I’ll start with a few of the more common activities that I don’t track (and why):
Steps per day. Although the recommendation to walk 10,000 steps per day is an arbitrary number, I do find that it is an excellent suggested baseline level of activity for most people. However, since I’m a fairly active person that exercises most days of the week (and even uses a standing desk at work and at home), I don’t find that this has any correlation with my fitness level.
Bodyweight. I’m fortunate enough that my bodyweight has varied little throughout my life. I credit this mostly to exercise (primarily strength training since my teenage years), along with generally watching my diet. Certainly, if my bodyweight would increase (especially in the form of adipose tissue), this would quickly become one of my KPIs.
Calories. In recent years, increased importance on the type of foods that we eat has been recognized. While the total energy that we consume certainly matters, the effects of different types of food also clearly play an important role. In other words, you would expect your body to react differently to 2,000 calories of pure sugar versus 2,000 calories of grass-fed steak.
Activities that I track (and how):
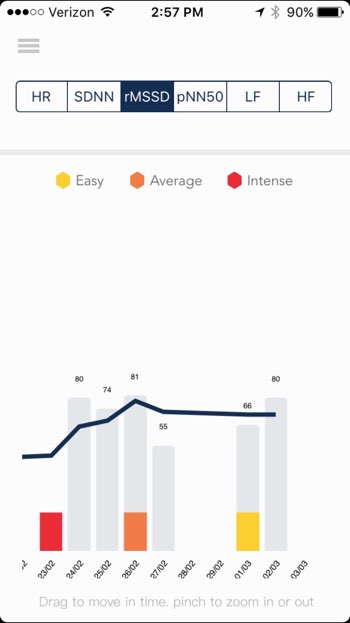
Heart Rate Variability (HRV). HRV is a measure of how much beat-by-beat variation occurs in your heart rate, which is governed by the balance of sympathetic and parasympathetic nerve activity. More simplistically speaking, HRV can give a sense of how much stress the body feels at a given time. (PDF of a review here). In a fully rested/low stress state, you should have a high HRV, and under conditions of high stress, you would expect your HRV to decrease. Increasingly, high level athletes are using measure of HRV to titrate their level of training for the day.
I use an app called HRV4Training (App Store) to track my HRV most mornings, which uses the iPhone camera and flash to measure your heart rate via plethysmography with surprisingly good accuracy (especially if used in a dark room). After this, your HRV can be viewed in the form of rMSSD (the unit by which HRV is calculated, called the Root Mean Square of the Successive Differences).
In my case, whenever my HRV rMSSD is above 80, I’m fairly well rested (which means I’ll probably do deadlifts that day).
I’ve found that my HRV seems to most strongly increase with the amount of perceived rest that I get, with frequent moderate-high level exercise, and with meditation. My HRV seems to decrease the most when I’m sleep deprived, when I’m sick (or feeling like I might be getting sick), or after overly intense exercise (especially too many deadlifts).
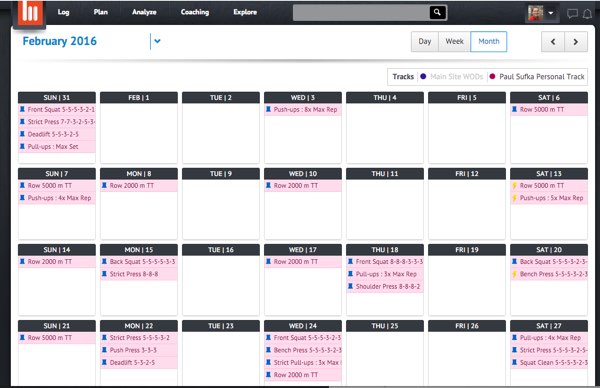
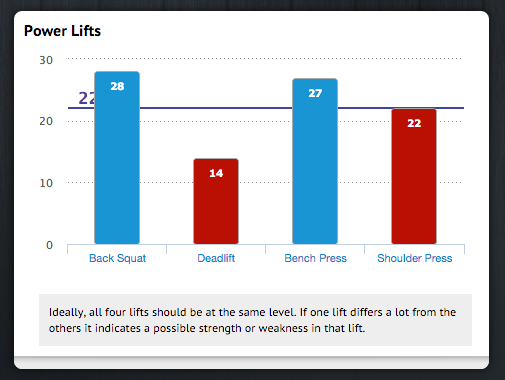
Exercise. I track exercise using a website called beyond the whiteboard, which is popular in the CrossFit community, and fits very well with the style of workout that I often perform. The site allows you to analyze your overall fitness level in comparison to other athletes who use the site, and also helps you identify strengths and weaknesses in your overall fitness.
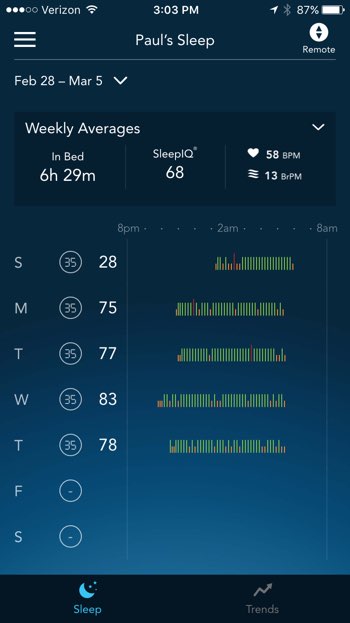
Sleep. I have a Sleep Number bed that has built in sleep tracking, although I don’t find that it always correlates with my perceived level of rest. Sometimes, this is because I’ll fall asleep in my son’s room while putting him to bed, so the data is wrong (such as on Sunday of the picture below).
Meditation. Over time, I’ve come to find a great deal of benefit from meditation (and I’ll give Dr. Ronan Kavanagh credit for initially turning my onto the idea of it.) I currently try to meditate 10–20 minutes each morning using the Headspace app (Web | App Store), and have felt increased ability to focus and generally calmer.
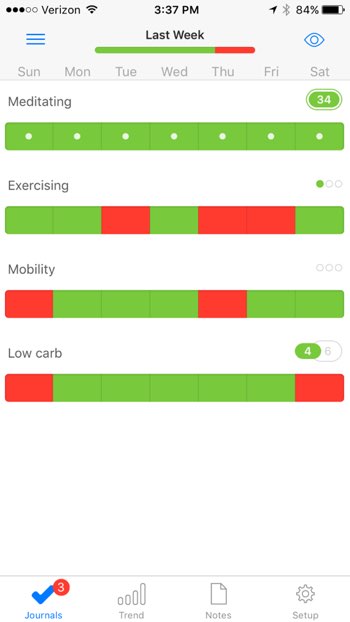
Other: Mobility & Diet. I use an app called Way of Life (App Store) to get a big picture view of a few things I’m tracking, such as meditation and exercise, and other things I’m trying to watch, such as doing some mobility work (especially hips, ankles, and shoulders) most days. The app essentially allows you to check yes or no for each day, and encourages you to go on a streak of 3+ days.
”We are what we repeatedly do. Excellence, then, is not an act, but a habit.” — Aristotle
#ACR15 marked the eighth consecutive American College of Rheumatology Annual Meeting that I have been fortunate enough to attend. I had the feeling of coming full circle, since the first ACR meeting I ever attended (when I was just a chief resident) was the 2008 meeting, also held in the wonderful city of San Francisco.
As I’ve mentioned numerous times before, since this meeting is the biggest thing in rheumatology each year, I spend some time thinking about how to optimize my time there, which results in an incredibly full schedule.
Review Course
”Scientific knowledge is a body of statements of varying degrees of certainty—some most unsure, some nearly sure, none absolutely certain.” — Richard Feynman
The pre-meeting ACR Review Course is an educational highlight for me each year. Personal favorites were the sessions on Central Nervous System Manifestations of Rheumatic Diseases and Extra-Pulmonary Manifestations of Sarcoidosis, although I’ll eventually need to repeat the A Rational Approach to Dermatology for the Rheumatologist on SessionSelect.
This year, as an alternative to tweeting out main points, I took notes on most of the sessions in Evernote and made them available publicly.
(I format my notes using Markdown, which combines readability with the ability to easily convert them to other formats. Highly suggested if you do any online writing).
Tech Med Track
“I’m interested in things that change the world or affect future in wondrous new technology where you see it and you’re like, ‘How did that even happen? How is that possible?’” — Elon Musk, Wait But Why: The Cook and the Chef: Musk’s Secret Sauce
We had another great Tweetup this year, and it was great to both catch up with friends from all over the world and finally meet a number of people in person. At the #ACR14 Tweetup, I had mentioned the article “You don’t have to be local,” that discusses the balance between being a local or a global person, and the Tweetup is a great way to keep this in balance, along with a great networking opportunity.
During the meeting we discussed plans to improve #RheumJC over the coming year, which will include expanding the organizing team. Keep an eye out for a more official call for anyone interested in helping.
Right now, the best way to make sure you don’t miss anything with #RheumJC is to sign up for our mailing list and to follow us on Twitter at @RheumJC.
Other Stuff You Shouldn’t Miss
Dr. Jonathan Hausmann (@hausmannMD) presented Use of Social Media By Rheumatology Fellows in North America (abstract #1012) showing that Twitter was used by a surprising low number of rheumatology fellows at 18%, hypothesizing: “It is possible that warnings about potential harms of social media within healthcare institutions have made rheumatology fellows less likely to engage on these platforms.” Given the strong benefit many of us have seen from the use of Twitter for ongoing education, I agree with suggesting further steps to “examinine the barriers to professional use of social media, as well as educate physicians about its potential benefits.”
Dr. Samuel Whittle (@samwhittle) presented Investigation of Environmental Associations of Fibromyalgia Pain Using Twitter Content Analysis (abstract #2296), using a novel method of analyzing Twitter user data: “Sentiment analysis, a computerized linguistic method that uses natural language processing and text analytics to identify subjective information … to quantify the affective content of each included tweet” and correlating this with weather data at the location of each individual tweet. Results showed that humidity increases were the only weather change associated with higher pain (r=0.009, p=0.001). More importantly, this abstract is an amazing example of the vast data available from social media for analysis.
The session on Wearable Biosensors to Advance Rheumatology, with talks on Wearable Biosensors and the Quantified Self Movement by Dr. Brennan Spiegel (@BrennanSpiegel) and Applying Biosensors to Advance Clinical and Research Settings in Rheumatology by Dr. Jeffery Curtis (@RADoctor)are both packed with cutting edge insights into how we (and our patients) will be using biosensors in the near future, and where this area may be going. I’ll have to take a second look at this one as well on SessionSelect.
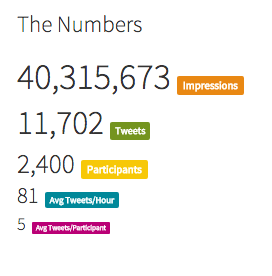
The work of CreakyJoints (@CreakyJoints) and Dr. John Cush’s RheumNow (@RheumNow), who are building excellent, evidence based, online communities and resources for patients and rheumatologists respectively. You’ll notice the influence they’ve had (especially @CreakyJoints) at #ACR15 in the statistics below.
Meeting with ABIM Regarding MOC
During the meeting, I volunteered to echo the frustrations of the social media world regarding MOC to the ABIM during a focus group (at 7:15am, no less).
Suffice it to say, we’re quite fortunate that the ACR so strongly supports it’s members with a well written position statement [pdf]. Thank you!
Please Don’t Interrupt: “It takes a while for our brains to get into a focused state where we’re able to concentrate fully on a task without feeling distracted.”
The Tweetup has become an yearly event at the American College of Rheumatology Annual Meeting, and the use of Twitter at medical conferences is now so ubiquitous that it is indexed and searchable on Symplur, which includes the meeting hashtag for this year: #ACR15.
Twitter has shown huge value in allowing individuals to build their own personal learning network, but nothing compares to forming and strengthening these connections in person at events like the Tweetup. (If you’re relatively introverted like me, I highly suggest this YouTube video on networking by Tim Ferriss: How to Rock SXSW in 4 Hours).
At this point, if you’re not using Twitter as a tool for lifelong learning, you’re missing out. Influential physicians such as Dr. Eric Topol (@EricTopol) have discussed how Twitter has helped him maximize his productivity, and the Dean of Harvard Medical School, Dr. Jeffrey Flier (@jflier), was recently profiled about the value of Twitter in the Wall Street Journal.
”We’ve reached a point where social media is now part of the professional workflow. While it’s a minority that understand and leverage these tools, the ones who are onboard are helping reshape the image of our organizations and our profession. Those of us creating, curating and conversing in the great wide open will continue to benefit from our public presence.”
If you’re new to Twitter, don’t worry. A quick primer can be found in last year’s ACR Social Media Bootcamp presentations:
The goal of the Tweetup is always to give people a chance to connect on the topic of social media in rheumatology and medicine. Every year, it leads me to new projects such as #RheumJC, the recently formed Rheumatology Twitter-Based Journal Club. I hope others find similar opportunities from attending.
Looking forward to seeing everyone at the Tweetup!







{kind=link}